
Managing Diabetes with Peer Mentoring
Organization : Center for Health Incentives and Behavioral Economics
Project Overview
Project Summary
To help lower their blood sugar levels, African American veterans with poor diabetes control were matched to peer mentors who had previously learned to manage their diabetes.
Impact
Mentored patients lowered their blood sugar levels by 1.1 percentage points, dropping from 9.8% to 8.7% over six months.
Source
Source
Challenge
In the United States, 29 million people have diabetes, a chronic disease that requires careful monitoring and management of blood sugar levels. However, many patients struggle to follow the regimens recommended by their doctors. At the Philadelphia Veterans Affairs Medical Center, the standard guidance provided to diabetic patients was to notify them of their blood sugar levels along with where their levels should be as per recommendations by the American Diabetes Association and Veteran’s Affairs. The challenges was to uncover ways to help patients who were having trouble managing the disease, taking into account the human tendencies that make long-term treatment difficult.
Design
Researchers paired African American veterans who persistently struggled with diabetes control with a peer mentor who had experienced a similar struggle, but had now learned to manage their disease. The patient and mentor were matched by race, gender, and age to invoke a sense of identity. The peer mentors completed a one-on-one training to learn their mentees’ stories, understand their motivations, identify their goals, and help them to create an achievement plan. Peer mentors were instructed to speak to their assigned patient at least once a week, which acted as a commitment device to keep patients on track with their plans and goals.
Excerpts from Guidelines Provided to Mentors
Impact
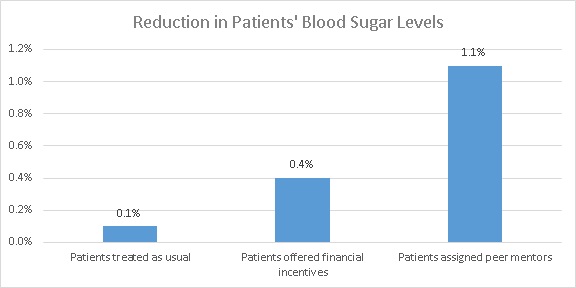
A randomized controlled trial found that, over the six-month study period, peer mentors helped patients reduce their blood glucose levels by 1.1 percentage points compared to patients receiving the standard care, dropping from 9.8% to 8.7% over a six month period.
Furthermore, patients who were assigned peer mentors experienced greater improvements than a group of patients who were offered financial incentives equivalent to $100 for reducing their blood sugar levels by one point, and $200 for reducing their blood sugar levels by two points, over the same six-month period. This suggests that invoking identity and using plan making and regular commitment calls can reduce blood sugar levels more effectively than money can.
Implementation Guidelines
Inspired to implement this design in your own work? Here are some things to think about before you get started:
- Are the behavioral drivers to the problem you are trying to solve similar to the ones described in the challenge section of this project?
- Is it feasible to adapt the design to address your problem?
- Could there be structural barriers at play that might keep the design from having the desired effect?
- Finally, we encourage you to make sure you monitor, test and take steps to iterate on designs often when either adapting them to a new context or scaling up to make sure they’re effective.
Additionally, consider the following insights from the design’s researcher:
- Connect patients with peer mentors who have similar backgrounds and who faced related health challenges.
- Create training programs to teach peer mentors strategies for understanding the patient’s needs and also how to determine effective ways to motivate patients. Training can be reinforced once per month.
- Provide the mentor with compensation in return for maintaining frequent (e.g. once per week) contact with the patient.
Cost effectiveness
- Mentors received $20 per month to call their mentees once a week.
- Because the peer mentor program only requires phone calls between patients and their mentors, it should be easily scalable and cost-effective.
Project Credits
Researchers:
Judith A. Long Contact Philadelphia Veterans Affairs Center for Health Equity Research and Promotion
Erica C. Jahnle University of Pennsylvania
Diane M. Richardson Philadelphia Veterans Affairs Center for Health Equity Research and Promotion
George Loewenstein Carnegie Mellon University
Kevin G. Volpp Philadelphia Veterans Affairs Center for Health Equity Research and Promotion
