
Free Lentils Can Boost Child Vaccination Rates
Organization : Innovations for Poverty Action
Project Overview
Project Summary
An NGO in India provided reliable immunization services with modest incentives—lentils and plates—to families for immunizing their young children.
Impact
Providing reliable immunization services with the small incentives increased the number of children who were fully immunized by 33 percentage points.
Cost
It cost $25 (1102 rupees) per immunization in villages that received both reliable immunization services and incentives. This was more cost effective (per immunization) than just increasing the reliability of immunization services ($56 per immunization).
Challenge
In India, immunization services are offered for free in public health facilities, but the immunization rate remains low in some areas. In the rural area where this study took place, only 2% of children were receiving the full package of immunizations, though a much larger percentage had started the package. This suggested that the barrier to immunization could be the opportunity cost of making multiple trips to the clinic. High absenteeism among health workers likely further deterred families from taking their children to complete their full immunization schedule.
Design
The NGO Seva Mandir used two approaches to increase full immunization rates in rural Rajasthan. One approach focused on establishing regular availability of immunization services through “immunization camps.” The camps consisted of a mobile immunization team, including a nurse and assistant, both hired by the NGO, who provided monthly immunization services in the villages. In each village a social worker was responsible for identifying children, informing mothers about the availability of the immunization camps, and educating them about the benefits of immunization.
The second approach involved providing the same immunization camps, but also offered parents 1 kg of raw lentils for each immunization administered to their child and a set of thalis (metal plates used for meals) upon completion of the child’s full immunization. The value of the lentils was about 40 rupees (or US$1), equivalent to three quarters of one day’s wage, and the value of the thalis was about 75 rupees. Seva Mandir decided to provide lentils, rather than cash, because the food was useful to the family and had immediate nutritional value. The amount roughly corresponds to the opportunity cost of time for the mother. The thalis were chosen as a tangible sign of achievement, while also being immediately useful.
Incentives aimed to increase the chance that families would immunize their children and complete the full vaccination schedule of five immunizations.
Vaccination and incentive schedule
1 – bag of lentils
2 – bag of lentils
3 – bag of lentils
4 – bag of lentils
5 – bag of lentils & set of plates
From 2004-2007, researchers conducted a randomized controlled trial to evaluate the impact of the two approaches on immunization rates in rural Rajasthan, India.
Impact
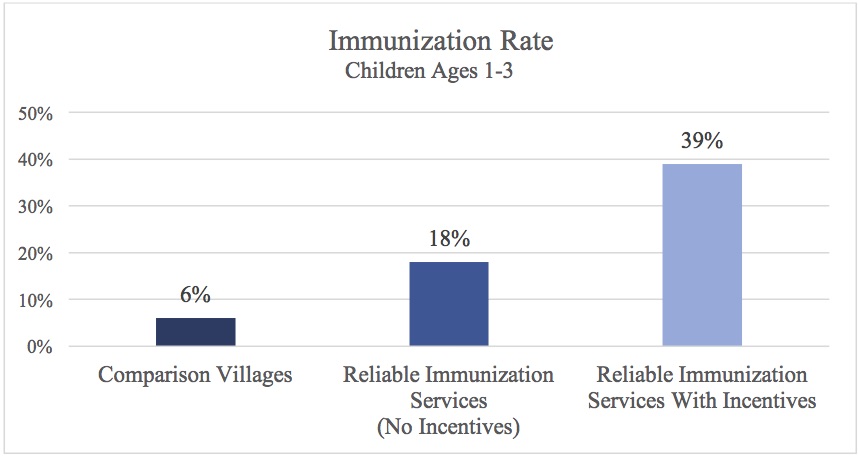
A randomized evaluation found that providing reliable immunization services with small incentives increased the rate of full immunization for children aged 1-3 by 33 percentage points, from 6% in comparison villages where immunization services were administered as usual to 39% in program villages. Villages that received reliable immunization services without incentives had an 18% rate of full immunization, a 12 percentage point increase relative to the comparison group.
Children in the surrounding areas of villages that received immunization camps and incentives were also more likely to be fully immunized than those in surrounding areas of villages that only received the camps.
What worked best?
- Providing incentives in combination with regular immunization services was much more effective and cost-effective than only providing regular immunization services.
Implementation Guidelines
Inspired to implement this design in your own work? Here are some things to think about before you get started:
- Are the behavioral drivers to the problem you are trying to solve similar to the ones described in the challenge section of this project?
- Is it feasible to adapt the design to address your problem?
- Could there be structural barriers at play that might keep the design from having the desired effect?
- Finally, we encourage you to make sure you monitor, test and take steps to iterate on designs often when either adapting them to a new context or scaling up to make sure they’re effective.
Additionally, consider the following insights from the design’s researcher:
Would this work elsewhere?
These approaches have only been tested in one context, in rural Rajasthan, India, under the implementation of an NGO that was known and trusted by the community. However, researchers believe that the impacts might be generalizable to other contexts where the same basic conditions exist: where parents want to vaccinate their children; where pre-existing services are unreliable; and where parents have trouble completing immunization schedules (i.e. data show that immunization rates are relatively high, and then taper off). Like with every intervention, effective implementation, in which incentives and vaccines are provided regularly and appropriately, would also be necessary for these approaches to work elsewhere.
Cost
In 2004-2007, the average cost per immunization was $56 (2202 rupees) in villages that received reliable services and $25 (1102 rupees) in villages that received reliable immunization services and incentives. When using existing public health infrastructure, the estimated average cost of fully immunizing a child is $25 in camps without incentives, and $17 in camps with incentives. Implementing the program with incentives was more cost-effective than implementing it without, because many of the fixed costs were the same, but more children attended camps with incentives (driving down the average cost per child).
Advice for Implementers
- The most cost-effective way to conduct immunization camps with incentives would be by using existing public health infrastructure. Many developing countries have an extensive public health infrastructure that is capable of conducting such regular immunization camps with incentives. In these contexts, the incentivized camps could piggy back on the existing health system with its sunk cost of staff and physical infrastructure for vaccines. In that case, the only costs would be for travel, medicine, monitoring, and the incentives themselves.
- At the same time, administering such a program within a large bureaucracy could be challenging. Effective implementation is key, and would require active monitoring.
Other reasons the program might have been so effective
- Trust: Seva Mandir had been active in the area for over 50 years and was trusted in villages. While the program was new, the organization thus benefitted from a high level of trust among villagers, which might have ameliorated issues of mistrust that surround immunization programs in India.
- Effective implementation and monitoring: At the first immunization, every child was given an official immunization card indicating their name, the name of their parent/s, and the date and type of each immunization performed. The nurse also kept a detailed logbook. The presence of the nurse and assistant was verified by the requirement of timed and dated pictures of them in the villages and by regular monitoring. Review of records showed that of 1336 planned camps, 95 percent (1269) took place.
Project Credits
Researchers:
Abhijit Banerjee Massachusetts Institute of Technology
Esther Duflo Contact Massachusetts Institute of Technology
Rachel Glennerster Abdul Latif Jameel Poverty Action Lab (J-PAL), Massachusetts Institute of Technology
Dhruva Kothari Columbia University
